 Book Now
Book NowIndividual problems demand individualized solutions.
Personal preferences demand personal understanding.
Successful results demand successful planning and execution.
Patients with mismatched size and/or shape of breasts, with tubular / tuberous breast features, and/or with inverted nipples often suffer immensely, and appeal for a corrective procedure. Expert help is available.

Dr. Laverson approaches the patient with breast mismatch (asymmetry between right and left sides) by finding out which breast the woman likes most. If there are problems with size and/or shape, these are identified, discussed, and suitable improvement planned. Adjustments to her favorite breast are most predictable. The favorite breast is the one requiring the least surgery. Features on the better side are anticipated before surgery, and measured both before and during surgery: Breast width, nipple level, the bottom of the breast, and breast volume. These measurements are matched on the opposite side. A procedure combining breast augmentation, breast reduction, and/or breast lift techniques is designed for the least favorite side so that both right and left breasts will be closer in size, shape, and appearance to one another. Computer simulation with implants is useful for selection of the best size for women with asymmetry. Several results for women with asymmetric breasts shown HERE.
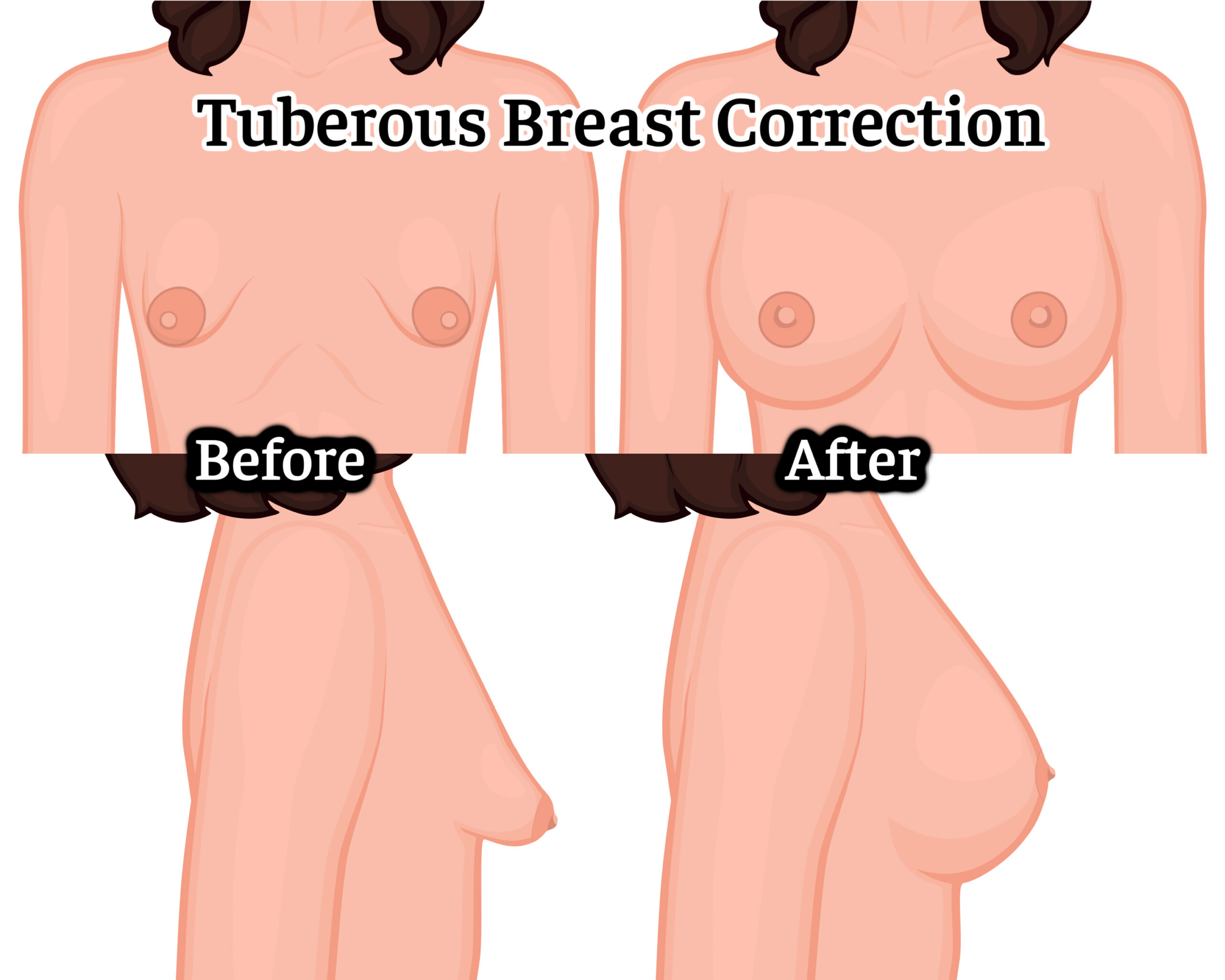 Tuberous or “tubular” breasts manifest in many ways. Most often, only mild features are present, such as a high infra-mammary crease, or narrow breast base width. These are best improved by re-shaping the breast from the inside with a carefully chosen breast implant. Additionally, Dr. Laverson re-distributes breast tissue over the implant to uniformly broaden the breast base and to nicely lower the infra-mammary fold (crease at the bottom of the breast), creating a robust shape. Excess centralization of breast glandular tissue behind the nipple and a large “puffy” or protuberant areola (pigmented skin around the nipple) are present in breasts with more obvious tuberous form. These findings are managed by peri-areolar “purse string” breast lift and areola reduction techniques. The results are refined as necessary to achieve the most beautiful result. Often, the outcome is dramatic, and transformational. It is not uncommon that a second or even a third surgical procedure, often minor, is required to further improve breast appearance, symmetry, scars, or treat implant related issues.
Tuberous or “tubular” breasts manifest in many ways. Most often, only mild features are present, such as a high infra-mammary crease, or narrow breast base width. These are best improved by re-shaping the breast from the inside with a carefully chosen breast implant. Additionally, Dr. Laverson re-distributes breast tissue over the implant to uniformly broaden the breast base and to nicely lower the infra-mammary fold (crease at the bottom of the breast), creating a robust shape. Excess centralization of breast glandular tissue behind the nipple and a large “puffy” or protuberant areola (pigmented skin around the nipple) are present in breasts with more obvious tuberous form. These findings are managed by peri-areolar “purse string” breast lift and areola reduction techniques. The results are refined as necessary to achieve the most beautiful result. Often, the outcome is dramatic, and transformational. It is not uncommon that a second or even a third surgical procedure, often minor, is required to further improve breast appearance, symmetry, scars, or treat implant related issues.
Nipple inversion is another condition that presents to variable degrees. One or both sides may be involved. Often, one side seems more severely affected. Nipple inversion is thought due to relatively shortened or tethered ducts and/or fibrous tissue around major ducts. Mild inversion may be present only intermittently. Sometimes, manual eversion will keep the nipples projecting normally for long periods of time. Disposition of the nipples may be temperature sensitive. In more severe cases, nipples are continuously inverted. Manual eversion may be difficult, then instantly and spontaneously reverses. Inverted nipples may evert during pregnancy as estrogen responsive breast ducts grow and elongate. In cases of persistent nipple inversion, an office surgical procedure everts the nipples permanently. Sometimes, nipple eversion requires stretching and complete, permanent, division of major breast ducts. The potential for lactation (breast feeding) from the involved breast may be permanently sacrificed. Breasts with advanced nipple inversion may not be satisfactory to nurse an infant. Pumping the breast for bottle feeding may be possible with inverted nipple(s). Nursing and/or pumping the breasts successfully may not be possible following surgical nipple eversion. Nipple sensation may be diminished after the eversion procedure, but areola sensation should remain.











